Liquid injectable Silicone (LIS) has been used for decades as a permanent filler for soft tissue augmentation in many locations to include the face, lips, eyelids, buttocks, hips and penis. LIS has a chemical composition of dimethyl polysiloxane. Pure LIS is nontoxic, noncarcinogenic, chemically inert and does not support the growth of microorganisms. It has never been approved for use as a soft tissue filler in the United States but is approved by the FDA for intraocular injection and is being used off-label as a filler for facial rhytides and in investigational protocols for human immunodefeciency virus-related lipoatrophy and severe facial deformities. There is enormous controversy about the safety of silicone. Most of the medical complications are a direct result of injection of massive volumes of impure, questionable-grade, adulterated silicone into the breasts, buttocks, hips and legs performed by unqualified, and even qualified persons in nonmedical facilities within the United States. Proponents argue that when purified sterile LIS is injected by trained professionals utilizing a minute volumes microdroplet serial puncture technique at appropriate intervals there is little risk. Opponents contend that liquid silicone is a “time bomb” and that disastrous, uncorrectable complications can occur despite good technique, good material and small amounts of injected filler (click HERE). I present a case of LIS granulomas developing after injection of medical grade LIS administered by a trained medical professional in Mexico.
A 64 year-old female presents for evaluation of a “rash” involving both legs, proximal thighs. The eruption began a few weeks before her appointment and she notes a “burning sensation” to the areas. She notes a history of silicone injections performed some 30 years ago in Mexico by a medical professional. She was instructed to go to a drug store and purchase cans of medical grade silicone for the injections. She notes she had around three sessions injecting into her hip and thigh regions. She states she was very thin and had bony hips. The injections softened her appearance.
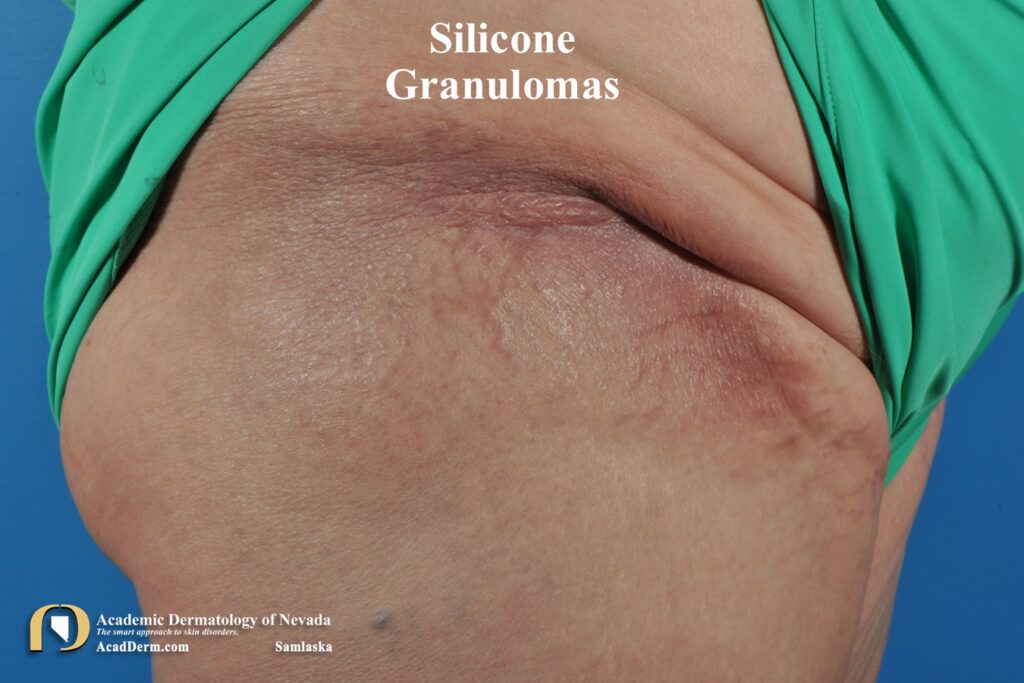
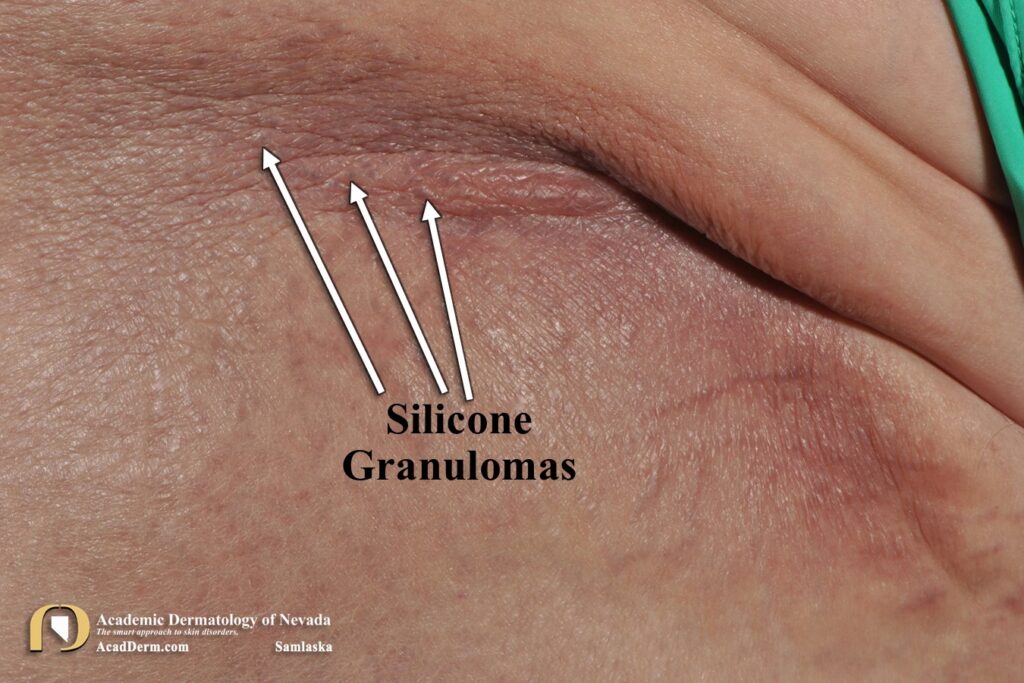
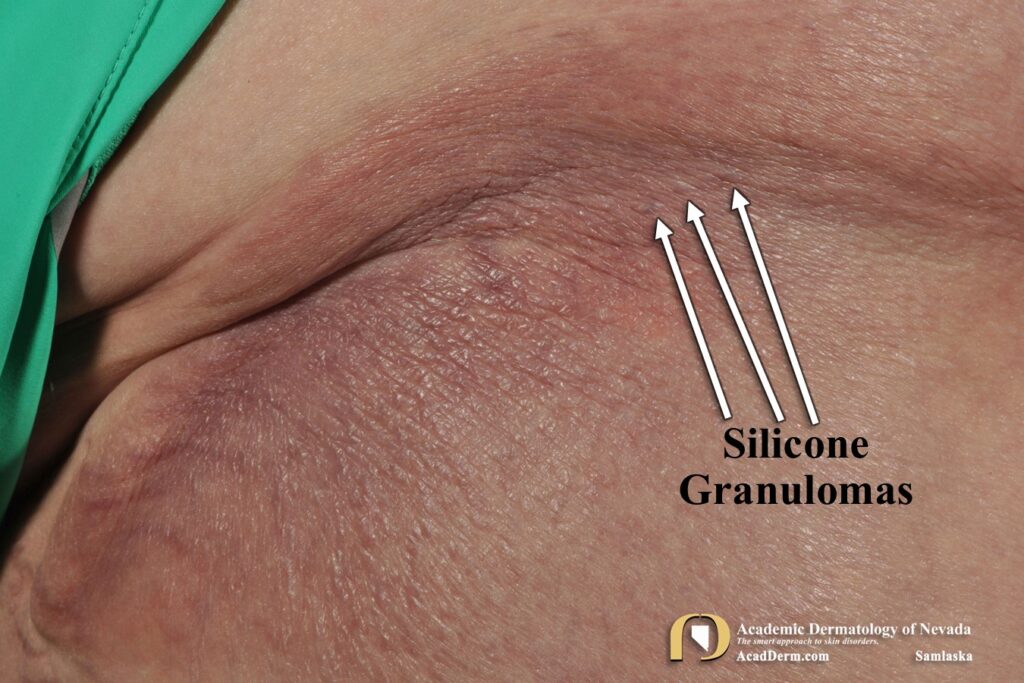
On clinical examination there was dramatic induration to the proximal thigh regions bilaterally (photograph above). Even more impressive were indurated plaques along both hip regions, demonstrating bluish papules with a somewhat vesicular appearance (photographs below). A punch biopsy was performed.

HISTOLOGY: The biopsy demonstrated multi-vacuolated histiocytic cells both scattered individual as well as aggregates, containing clear and somewhat refractile material. PAS special stains were negative for fungal elements. The features are consistent with the diagnosis of silicone granulomas.
Fascinating case. You can see the globules of silicone migrating to the dermal-epidermal junction producing these fine, vesicular-papules that coalesce into larger indurated plaques. The blue appearance is related to the Tyndall effect of light passing through the silicone and refracting out the bluish color. You can see the globules of silicone just under the surface of the skin.
COMPLICATIONS: The reason for many complications or even the development of granulomas remains a mystery. Some patients may be susceptible, or it may be a function of just too much LIS too fast, and/or too short of intervals. Many patients can develop acute symptoms to include shortness of breath and neurologic symptoms, promoting visits to the emergency room…a direct result of intra-arterial LIS being distributed to the heart, lungs and possible brain…not good. Patients are susceptible to recurrent infections, hypersensitivity reactions, permanent disfigurement and even death. Renal failure has been reported. To read more about severe complications click HERE.
TREATMENT: A diverse spectrum of therapies have been utilized to treat LIS granulomas to include minocycline, hydroxychloroquine, intralesional kenalog, low-dose isotretinoin, systemic steroids, and TNF inhibitors such as enbrel or humira. Ablative CO2 fractional laser and nonablative Erbium-glass lasers may be effective in some cases. Surgical intervention may be required in severe cases with systemic complications such as renal failure. Complete removal is impossible and the best one can hope for is to reduce the physical burden of the LIS.
Despite these risks, there is a growing trend of illicit cosmetic surgery being performed with nonmedical grade injectable silicone in the United States and abroad. Many of these unlicensed and unskilled practitioners administer LIS in quasi-sterile environments–hotel rooms, homes and even garages. Why do people continue to place themselves at tremendous risks to have these procedures? The answer is multi-factorial, to include the need for people to respond to society’s definition of beauty and success and the cheaper costs. I believe another component is that many are unaware of the risks they are taking. The more information we can get out on the potential risks to these procedures the better our likelihood of convincing people not to take that risk. To read more about LIS induced granulomas click HERE, HERE and HERE.