Mycosis Fungoides (MF) is a malignant neoplasm of T-lymphoytes, particularly of T-helper (Th) cells. The incidence is around 1 in 300,000 each year, but this number is rising. MF affects all races, however, in the United States black persons are more often affected than Caucasians.


The clinical features are variable depending on the various stages and at times may be confused with psoriasis. In the early patch/plaque stage the lesions are macular or slight plaques varying in size from 1-5 cm, but may be larger. Follicular variants may be confused with lichen nitidus. The eruption is often generalized, but often begins at a single site that spreads, often starting on the lower abdomen, buttocks, upper thighs, and breasts of women. The lesions may be atrophic or present with poikilodermatous features–mottled dyspigmentation and telangeictasias. In general the patch stage resemble eczema but uncommon forms may manifest as verrucous, hyperkeratotic, hypopigmented, purpuric, vesicular, bullous and pustular forms.


In the plaque stage the lesions are infiltrative and may resemble psoriasis, a subacute dermatitis or a granulomatous disorder such as granuloma annulare (see above). As the plaques progress they may coalesce into larger plaques and become confluent. In advanced disease the lesions may be painful and superficial ulcerations can develop. Enlarged lymph nodes often develop and are nontender, firm and freely mobile.
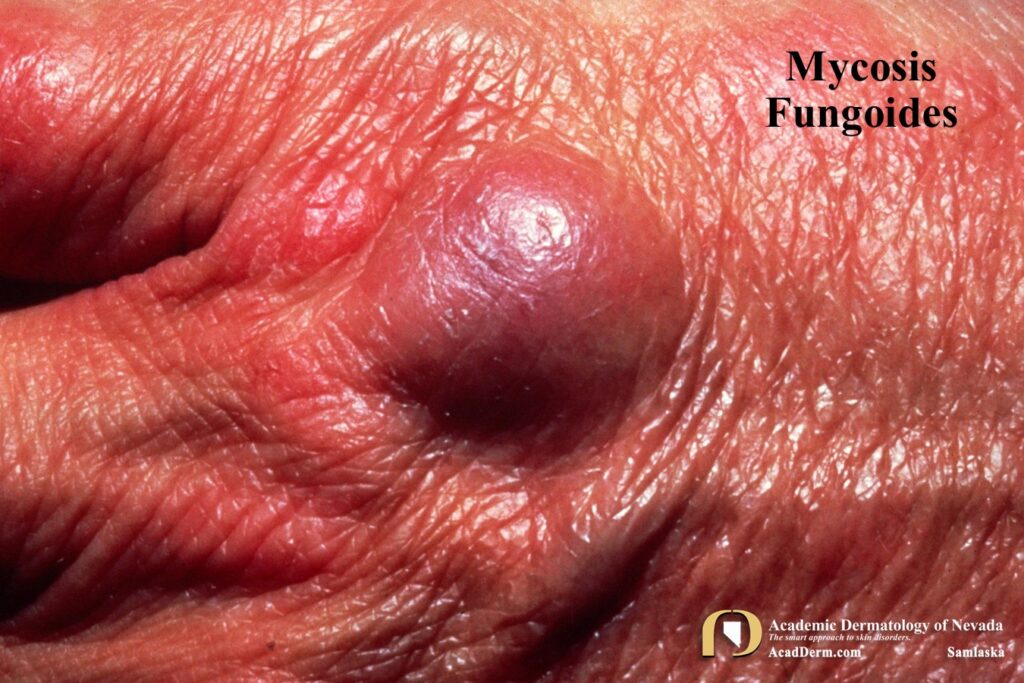
The tumor stage is characterized by large, variously sized and shaped nodules–infiltrative plaques which may break down to form deep oval ulcers with a necrotic grayish substance with rolled edges. The lesions have a predilection for the trunk. The erythematous form is a generalized exfoliative process that falls in the category of a erythroderma, which has many causes that often are much more acute. Erythroderma associated with MF is chronic and progressive.
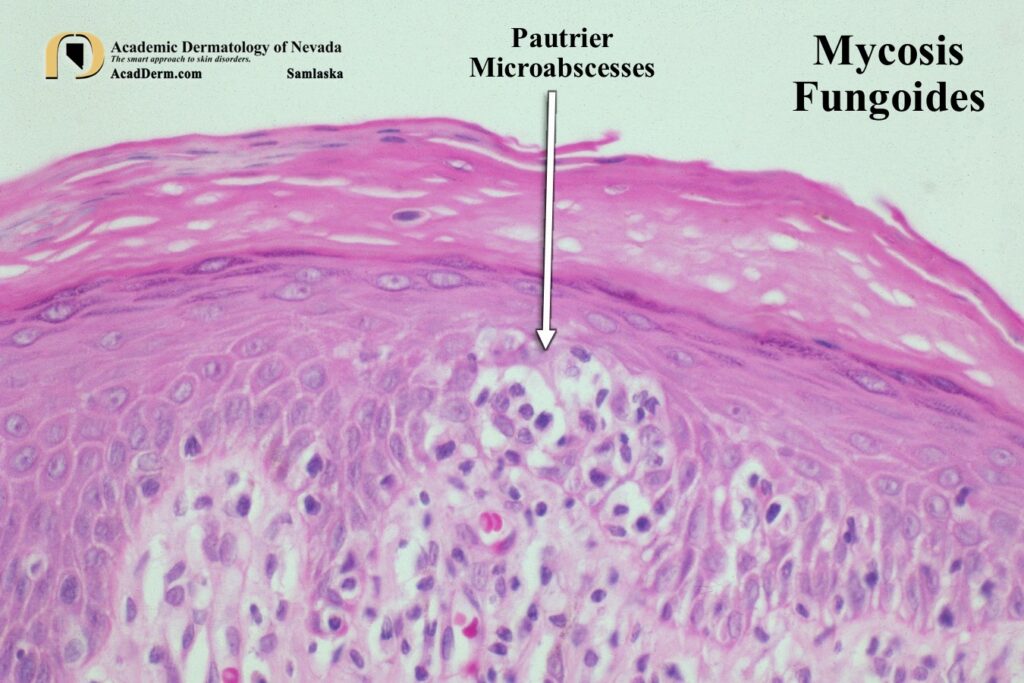
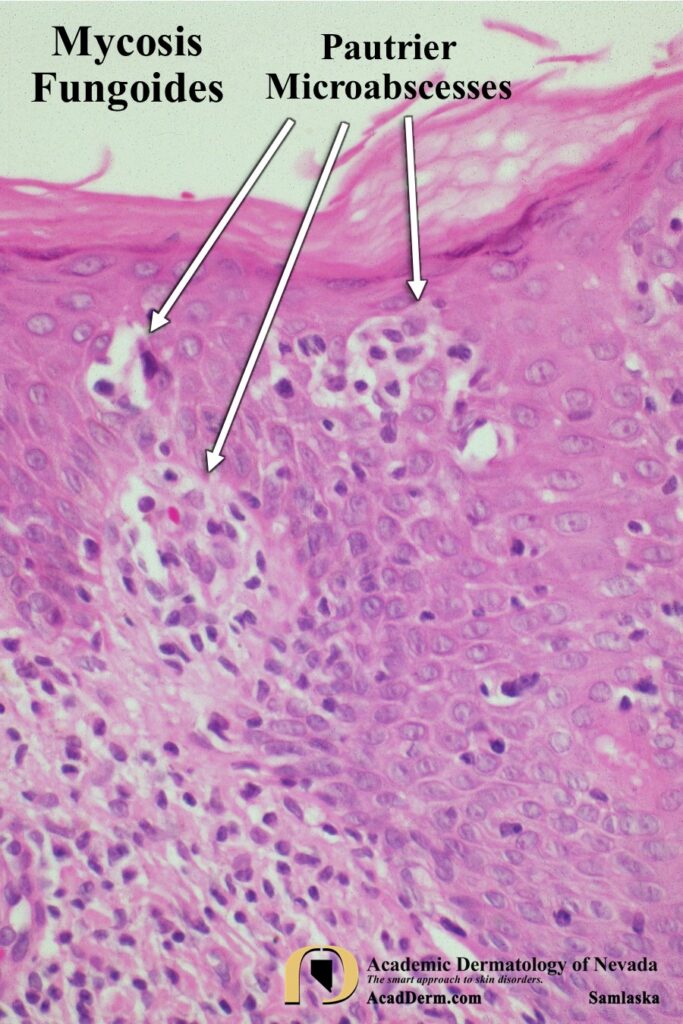
HISTOPATHOLOGY: Characteristic features on histology include: 1) Solitary or small groups of lymphocytes in the basal cell layer (Pautrier microabscesses), epidermotropism of lymphocytes with disproportionately scant spongiosis and papillary dermal fibrosis with bundles of collagen arranged haphazardly.
TREATMENTS: Detailed treatments are beyond the scope of this post. These patients are managed at sometimes by dermatologists but for tumor stage disease patients are manage by oncologists. The treatments range from topical steroids, topical nitrogen mustard, topical BCNU, ultraviolet therapy, PUVA, radiation, biologic response modifiers (immunotherapy), retinoids, systemic chemotherapy and fusion toxin. To read more about MF go HERE, HERE and HERE.