An ode to Jimmy Buffett…I have been getting a lot of questions from patients about this extremely rare malignancy. In my entire career I have only had 3 to 4 cases. Merkel Cell Carcinoma (MCC) was originally described by Toker in 1972. The cell of origin is the Merkel cell, which is a slow-acting mechanoreceptor located in the basal layer of the epidermis. The incidence is about 0.44 per 100,000 patient population, however, it has been noted that over the past 15 years more patients have been reported, and the incidence is believed to be increasing by about 8% per year. It is a malignancy of the elderly with 90% of cases older than 50, 76% are over 65 and 72% are over the age of 70. The mean age is 76 for women and 74 for men…95% occur in Caucasians.
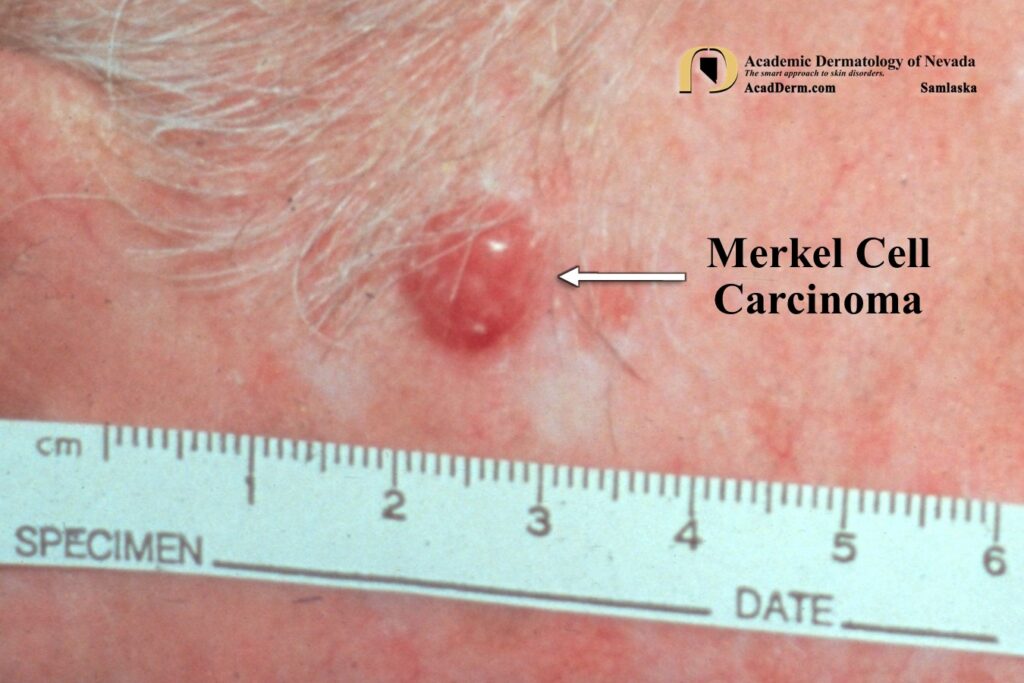


There is strong evidence that MCC is directly linked to sun exposure. Clinically the tumors present as a rapidly growing, nontender, red to violaceous nodule with a shiny surface and overlying telangiectasias. About 90% of cases occur on sun-exposed sites, particularly the head and neck regions. Most cases are not considered malignant at the time of biopsy. MCC are extremely aggressive tumors with a propensity for local recurrence and nodal and distant metastasis. MCC may be associated with immunosuppression, such as in patients with organ transplants, chronic lymphocytic leukemia and HIV infection. About one third of cases have regional lymph node involvement. Another third will eventually experience hematogenous spread. Spontaneous remission have been reported, most commonly in women with immunosuppression, secondary to management of the iatrogenic immunosuppression.
The Merkel Cell Polyomavirus (MCPyV) is associated with 80% of MCCs in North America and 25% of MCCs in Australia. MCPyV is a widespread viral infection with seropoprevalence in 30% of children under 5 to almost 80% in persons older than 50. The degree of involvement in promoting MCC as well as other cutaneous malignancies, such as Bowen’s disease, Basal Cell carcinomas (BCC) and Squamous Cell Carcinomas (SCC) has yet to be delineated.
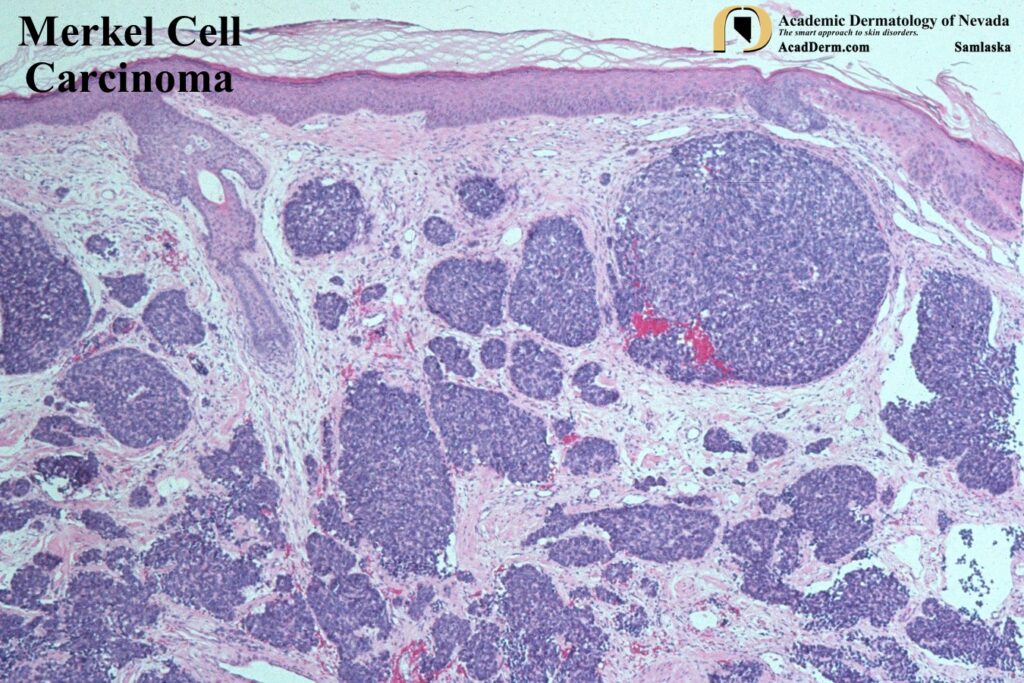
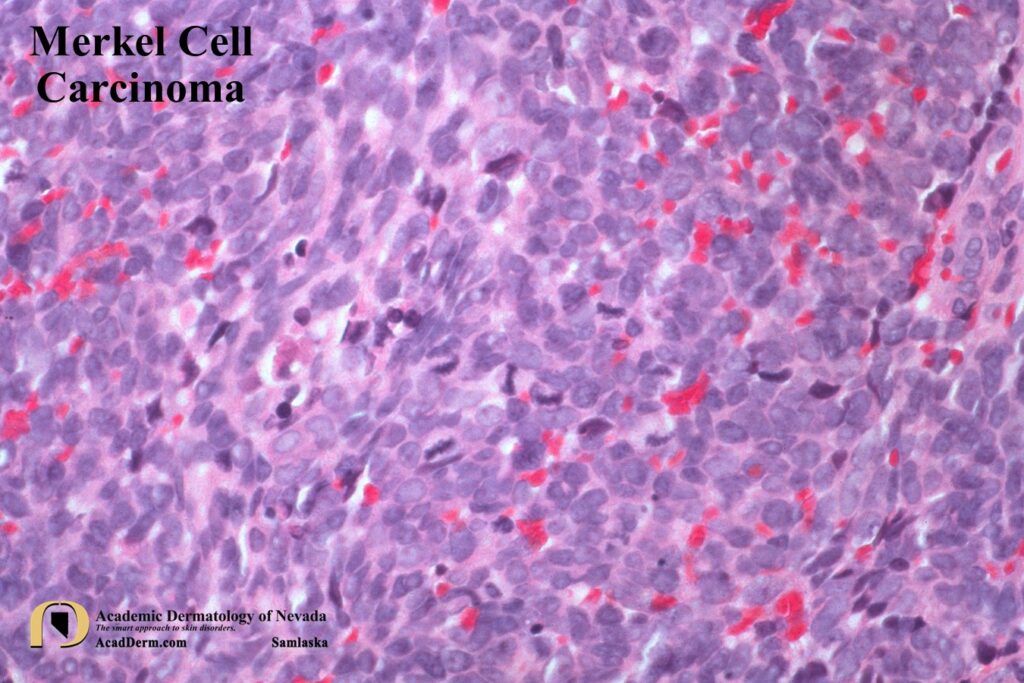
HISTOLOGY: It has been proposed by some to use the terminology Murky Cell Carcinoma referring to the “Murky” histologic pattern observed in MCC. It has also been referred to as a Neuroendocrine Carcinoma of the Skin and Merkeloma. To read more about this please click HERE. MCC is a dermal tumor that may extend into the subcutaneous tissue. The cells have very scant cytoplasm and hyperchromatic nuclei with a distinctive smudged (murky) chromatin pattern. Mitosis and apoptotic cells are often numerous. The cells are often arranged in sheets and cords. MCC must be differentiated from small cell lung cancer, Ewing sarcoma, melanoma and even BCCs. MCC are most commonly CK20 positive (perinuclear pattern), thyroid transcription factor 1 (TTF-1) negative, S-100 negative and leukocyte common antigen (LCA) negative. CK7 tends to be positive for small cell lung cancers but not MCC.
EVALUATION & PROGNOSIS: Staging is required to predict prognosis and guide therapy. Sentinel lymph node biopsy (SLNB) should be performed at the time of excision of the primary malignancy. One third of patients with no palpable adenopathy have a positive SLNB. CT scans are often positive for metastatic disease in 20% of patients. Even with small lesions under 1 cm in diameter metastatic disease may be found. PET scans or MRI scans should be performed. Palpable lymph nodes must be sampled for metastasis. Patients that are MCPyV positive have a better prognosis (45% versus 15% 5-year survival) and present on an extremity.
TREATMENT: Therapy will need to be individualized, pending extent of disease and presence or absence of metastasis. The initial goal, when possible, is to clear local disease. Surgical excision with wide margins followed with SLNB is key for patients without direct evidence of metastasis. Primary (for patients that can not tolerate surgery) and post-surgical excision radiation therapy may be helpful. Even after Mohs surgery, radiation therapy is recommended. Regional recurrence may occur, even after aggressive management and is a poor prognostic sign. Adjuvant chemotherapy has been disappointing and does not prevent later development of metastatic, regional, or local disease…it is not recommended. MCC may respond to chemotherapy, but disease progression often occurs. Partial responses have been reported with the multikinase inhibitor, pazopanib. To read more about MCC click HERE, HERE and HERE.