Vasculitis is a direct result of inflamed blood vessels. The vast majority of cases of cutaneous Leukocytoclastic Vasculitis, also referred to as Small-Vessel Vasculitis (LCV) follow an acute infection or exposure to a new medication. Palpable Purpura is the hallmark of LCV, the lesions ranging from pinpoint to several centimeters in diameter.
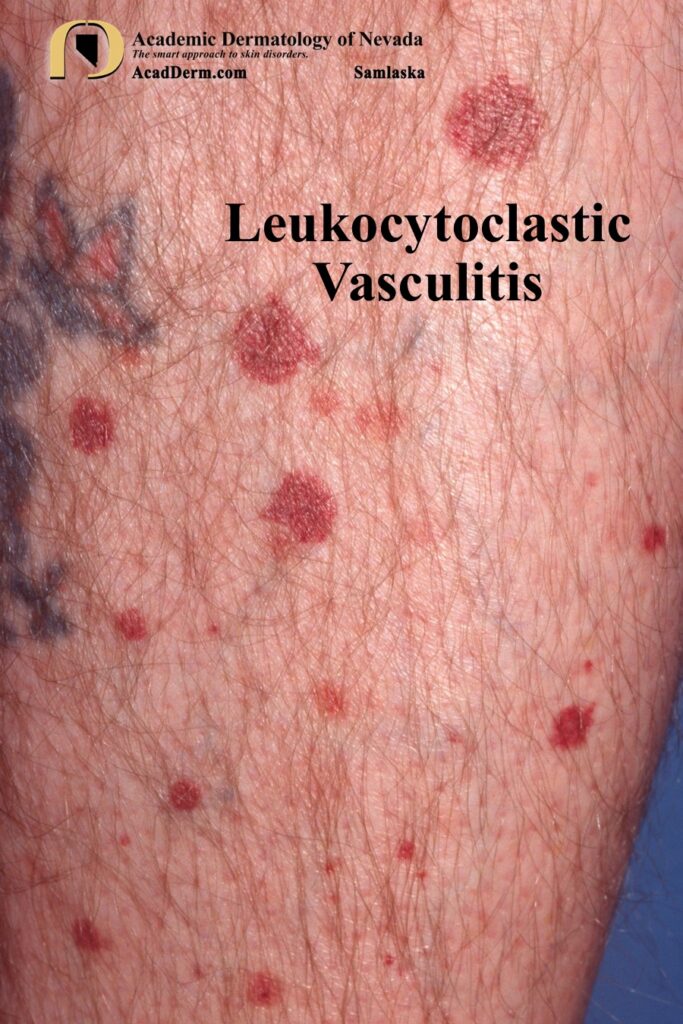
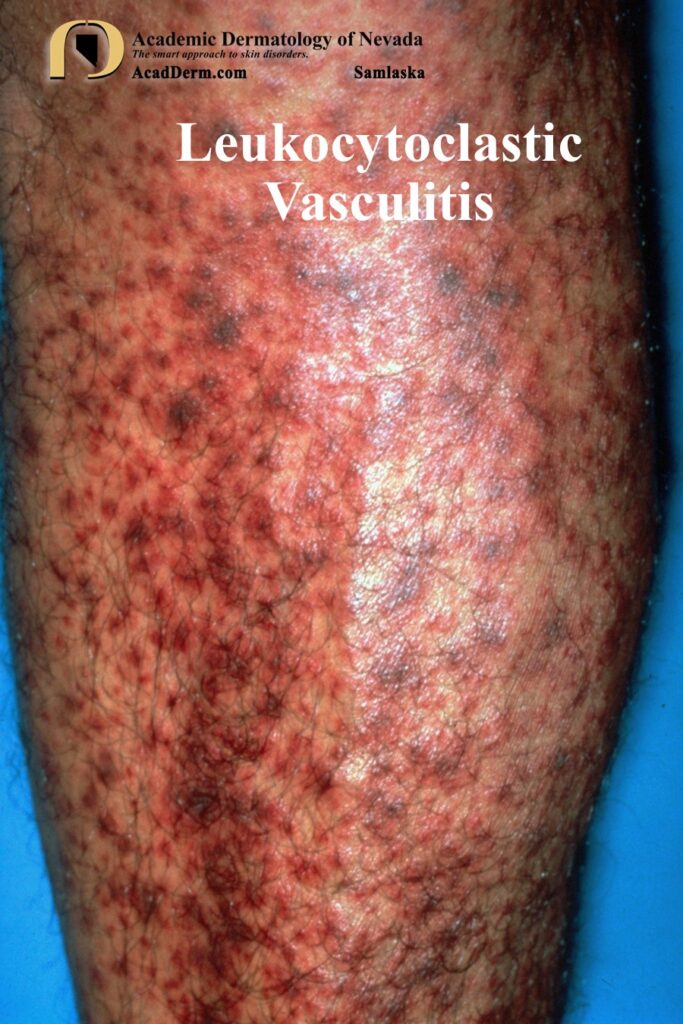

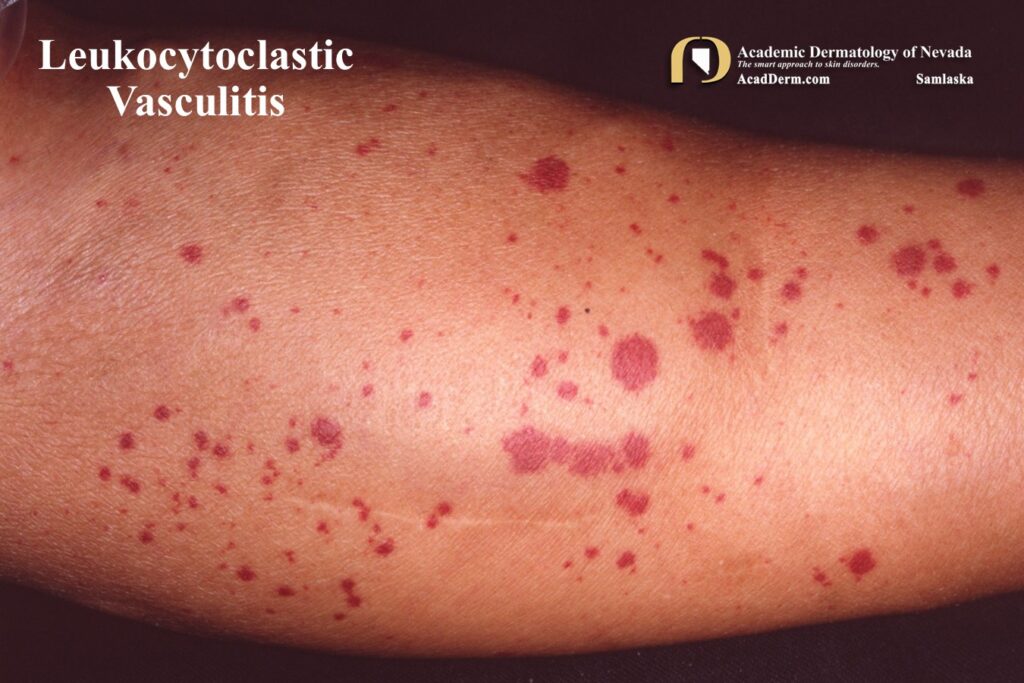
Annular, vesicular, bullous or pustular lesions have all been reported. There may be small ulcerations. Lesions predominate on the ankles and lower legs, affecting mainly dependent areas or areas under local pressure. Edema, especially of the ankles and lower legs may occur. Mild pruritus, fever and malaise frequently occur as can arthralgias, and less often, frank arthritis. The lesions usually resolve in 3-4 weeks and may leave postinflammatory hyperpigmentation. The arms may be involved, as demonstrate in the renal dialysis patient shown below.


Classification of Cutaneous small-vessel (postcapillary venule) Vasculitis:
A. Idiopathic cutaneous
B. Henoch-Schonlein Purpura
C. Acute Hemorrhagic Edema of Infancy
D. Urticarial Vasculitis
E. Cryoglobulinemic Vasculitis
F. Erythema Elevatum Diutinum
G. Granuloma Faciale
H. Other: drug-induced (antibiotics, thiazide diuretics, phenytoin, allopurinol, oral anticoagulants, ciprofloxacin and NSAIDs, malignancy (lymphoreticular & solid tumor, (connective tissue diseases, bowel-associated dermatitis-arthritis syndrome [bowel bypass]), HIV, and neutrophilic dermatoses (Behcet, Sweets, erythema nodosum leprosum, septic vasculitis, autoinflammatory conditions-familial Mediterranean fever, and serum sickness)
HISTOLOGY: There is angiocentric segmental inflammation of the postcapillary venule, expansion of the vessel wall, fibrin deposition and infiltration by neutrophils that show nuclei fragmentation referred to as karyorrhexis or leukocytoclasia. Endothelial cell swelling may be observed and fibrinoid necrosis of the vessel walls is seen. Vascular thrombosis may be found. The presence of tissue eosinophilia favors a medication as a cause.
ETIOLOGY: LCV is believed to be caused by circulating immune complexes that lodge in the vessel walls and activate complement–damaging the blood vessels. In most cases the cause of cutaneous LCV is idiopathic–unknown. The next most common associations are drugs (see above) and postinfectious. A host of associated infectious agents include Beta-hemolytic Streptococcus group A, Mycoplasma and rarely Mycobacterium tuberculosis. Most recently, COVID-19 has been reported.
TREATMENT: Mostly supportive. Rest and leg elevation are recommended. If an underlying cause is identified, such as a medication or infection, appropriate action should be instituted (remove the drug and treat the underlying infection). In severe cases a number of treatment options are available, such as NSAIDs, colchicine, dapsone, oral antihistamines, systemic corticosteroids and azathiaprine. In the most severe cases tumor necrosis factor (TNF) inhibitors, rituximab and cyclosporine have been used with beneficial results. To read more about LCV click HERE, HERE and HERE.