Keloids are benign dermal fibroproliferative tumors with no malignant potential. The first description of abnormal scar formation in the form of Keloids was recorded in the Smith Papyrus regarding surgical techniques in Egypt around 1700 B.C. The actual term Keloid, means “crab claw” and was first coined by Alibert in 1806 in an attempt to illustrate the way lesions expand laterally from the original scar into normal tissue. This distinction differentiates Keloids from Hypertrophic scars…Hypertrophic scars by definition are thicker scars that do not expand beyond the site of original injury. Since that time physicians have characterized scars as Normal, Hypertrophic or Keloidal.


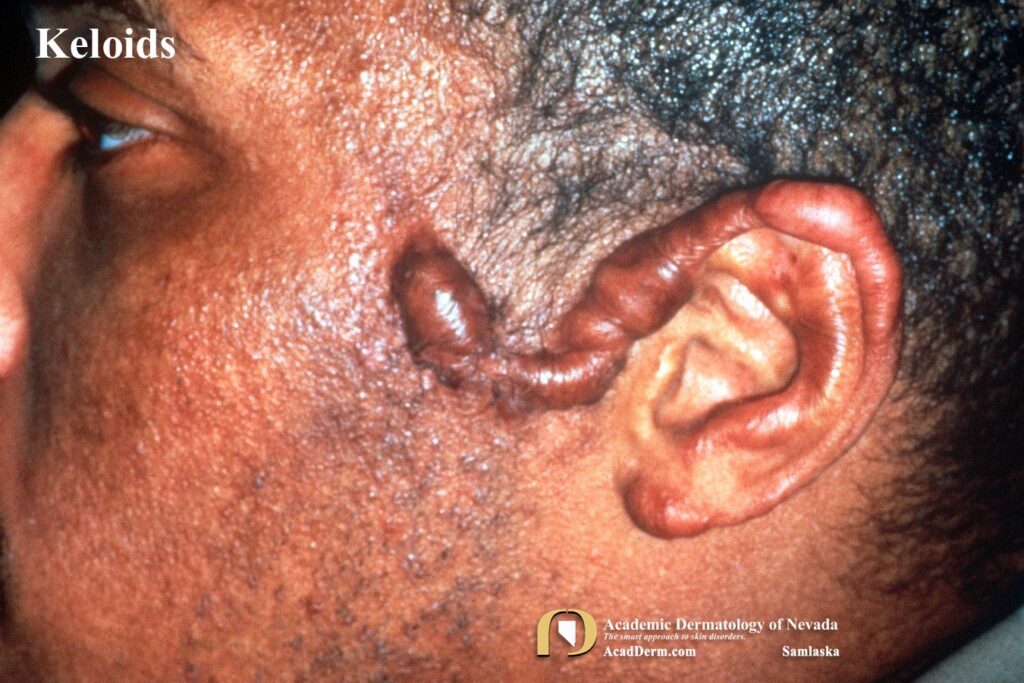
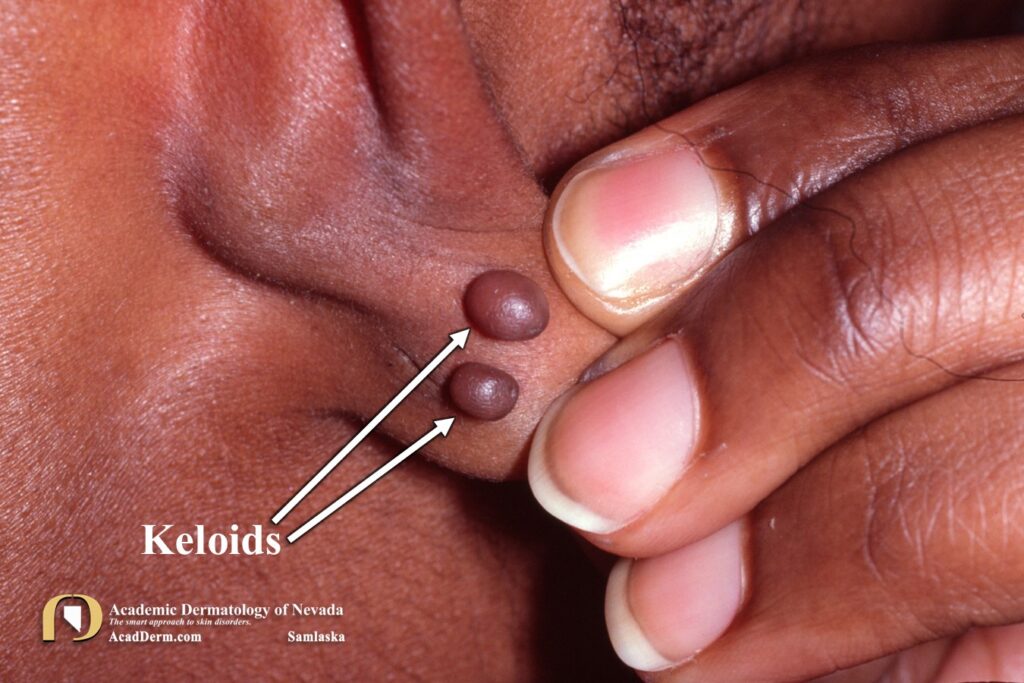
Keloids are firm, irregularly shaped, fibrous, hyperpigmented, pink or red excrescences. The growths usually arise as a result of a cut, laceration, or burn–or less often an acne pustules on the chest or upper back. The overlying epidermis is smooth, glossy, tender and thinned. Early on the lesions are red and tender with a consistency of rubber. It may be surrounded by an erythematous halo and may have telangiectasias. Some lesions may be tender, painful and pruritic. Rarely ulcerations or draining sinus tracts may occur.
The most common areas involved include the sternum, neck, ears, extremities and trunk. More rarely lesion may develop on the face, palms or soles. The earlobes are often involved and are directly related to ear piercing. Although keloids may occur in any ethnicity, black individuals are much more prone to developing Keloids.


Keloids are usually distinctive, and may be distinguished from hypertrophic scars by demonstrating clawlike projections which are not found in hypertrophic scars. Hypertophic scars may show signs of improvement over months of observation, but this does not occur with Keloidal scars, which tend to do the opposite and increase in size and thickness with time. Why certain individuals develop Keloids remains a mystery. Trauma is usually the immediate causative factor, but this induces Keloids only in those individuals with a predisposition for them.

HISTOLOGY: A Keloid demonstrates sharply defined nodular growths of myofibroblasts and collagen with a whorl like arrangement resembling hypertrophic scars. Centrally there is thickened hyalinized bundles of collagen which distinguishes Keloids from hypertrophic scars. Elastic tissue is scanty, as demonstrated in most scars. The pressure of the underlying tissue results in thinning of the normal papillary dermis and atrophy of adjacent appendages is frequently observed.
TREATMENT: Treatments are many and varied. I will frequently inject them with Kenalog in concentrations between 5 mg/cc to 10 mg/cc based on size and thickness. Rarely I use 20 mg/cc and even 40 mg/cc in large, pendulous lesions. These injections will need to be performed every month until the Keloid softens and flattens. Hopefully they respond well and once essentially flattened I extend the treatments out to every two months. Caution must be taken because the treatments can result in an atrophic scar if overdone, which is also problematic. Many of these scars will go dormant after many injections, what I called “burned out,” and the treatments can be discontinued. Other treatments can also be used individually or in combination with injections to include polyurethane or silicone patches, silicone gels, oral or topical tranilast, pressure dressings, surgical excisions followed up with Kenalog injections, intralesional 5-fluorouracil, intralesional botox, intralesional collagenase, oral verapamil, oral pentoxifylline, cryotherapy, superficial X-ray therapy, pulsed dye laser, carbon dioxide laser, needling and subcisions. The newest treatment option is JAK inhibitors such as tofacitinib and much excitement has been generated with the potential for this line of therapy. To read more about Keloids click HERE, HERE and HERE.