Kaposi Sarcoma (KS) was originally described by Moritz Kaposi in 1872 when he called it “multiple benign pigmented idiopathic hemorrhagic sarcoma.” Since those initial descriptions there have been three clinical presentations that have been referred to as “Classic form” or Old World KS: Initially KS was an indolent disease seen chiefly in middle-age men of Southern (bordering the Mediterranean) and Eastern European origin. Another variant involving African middle-aged males was reported in tropical Africa. A particularly aggressive form, known as African Lymphadnopathic KS has been reported to afflict young children under the age of 10 years.
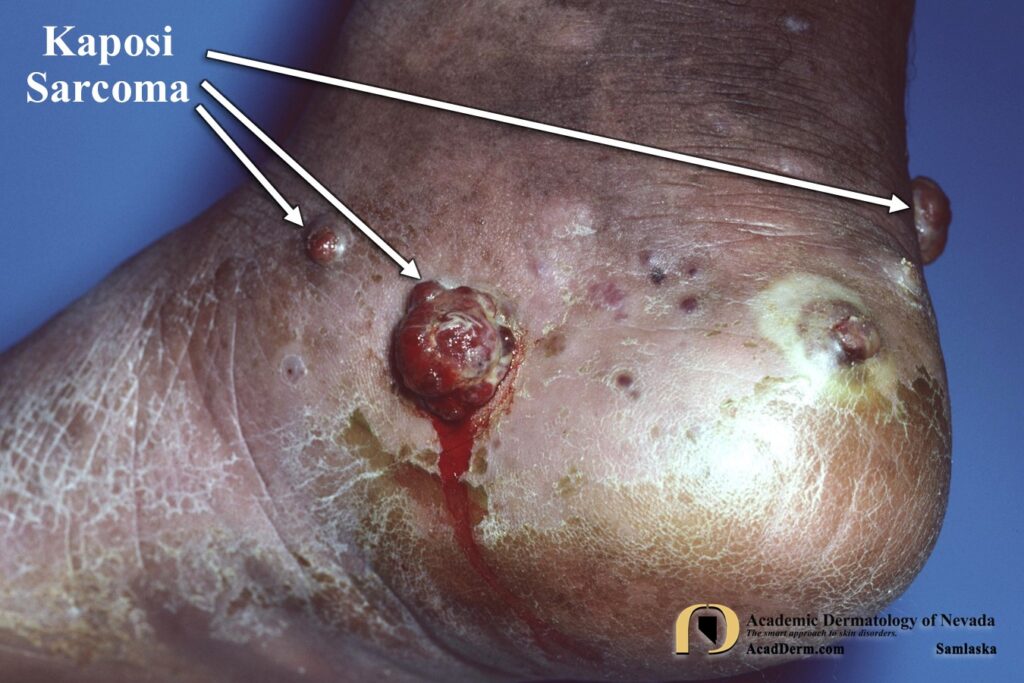
Patients with Classic KS develop early lesions on the toes and soles, presenting as reddish, violaceous, or bluish black macules and patches that spread and coalesce into nodules or plaques. These lesions often have a rubbery consistency. There may be some brawny edema of the affected leg. Subsequent macules or nodules may appear, usually much later, on the arms and hands and rarely may extend to the face, ears, trunk, genital or buccal cavity, especially the soft palate. The course is often slowly progressive and may lead to enlargement of the lower extremities resulting from lymphedema. Some patients may manifest periods of remission, particularly in the earlier stages. At times atrophic or hyperpigmented scars may appear.

In the 1980s AIDs or HIV disease exploded onto the scene and it wasn’t long before many of these patients were developing a new form of KS. At the time this was eventually referred to as New World KS, to distinguish it from the Classic or Old World forms. The clinical presentations for HIV associated KS was completely different, manifesting with one or several red to purple-red macules, rapidly progressing to papules, nodules, and plaques (See photos below). There is a predilection for the head, neck, trunk and mucosal surfaces. A fulminant, progressive course with nodal and systemic involvement is expected. KS may be the presenting manifestation of HIV infection. In HIV patients KS is considered by most to be a low-grade tumor associated with Kaposi sarcoma herpesvirus/human herpesvirus 8 (KSHV/HHV8) infection.



HISTOLOGY: KS may look different on histology depending on the stage of the disease. KS is a disease of blood vessels. Early lesions show irregularly shaped, ectatic blood vessels with scattered lymphocytes and plasma cells. The endothelial cells of the capillaries are large and protrude into the lumen, resembling buds. Later lesions show proliferation of vessels around preexisting vessels and adnexal structures, which may jut into the vascular space or lumen. Dull-pink globules, extravasated erythrocytes and hemosiderin are present. Nodular lesions are composed of spindle cells with erythrocytes that appear to line up between spindle cells with no apparent vascular space.
TREATMENT: All types of KS are radiosensitive and radiation therapy has been used with much success in early disease. Local excision, cryotherapy, alitretinoin gel (Panretin), locally injected chemotherapy or IFN and laser ablation have been used for unresponsive, localized lesions. Intralesional injections of vincristine solution, every two weeks for around 8 months may be useful. Systemic therapy using IFN, vinblastin, and actinomycin D have been used successfully. In patients with HIV associated KS patients respond to protease inhibitors which have been shown to produce antiangiogenic effects. However, non protease inhibitor therapy for KS also respond well to treatment, suggesting that the mechanism for overall improvement may be related to immune function and and not antiangiogenic mechanisms. For advanced KS Liposomal anthracyclines and paclitaxel have been used as first-line and second-line monotherapy respectively. New treatments for HIV associated KS continue to expand to include chick point inhibitors, VEGF/VEGF inhibitors, cART and NNRTI-based medications are currently under study. To read more about KS click HERE, HERE and HERE.