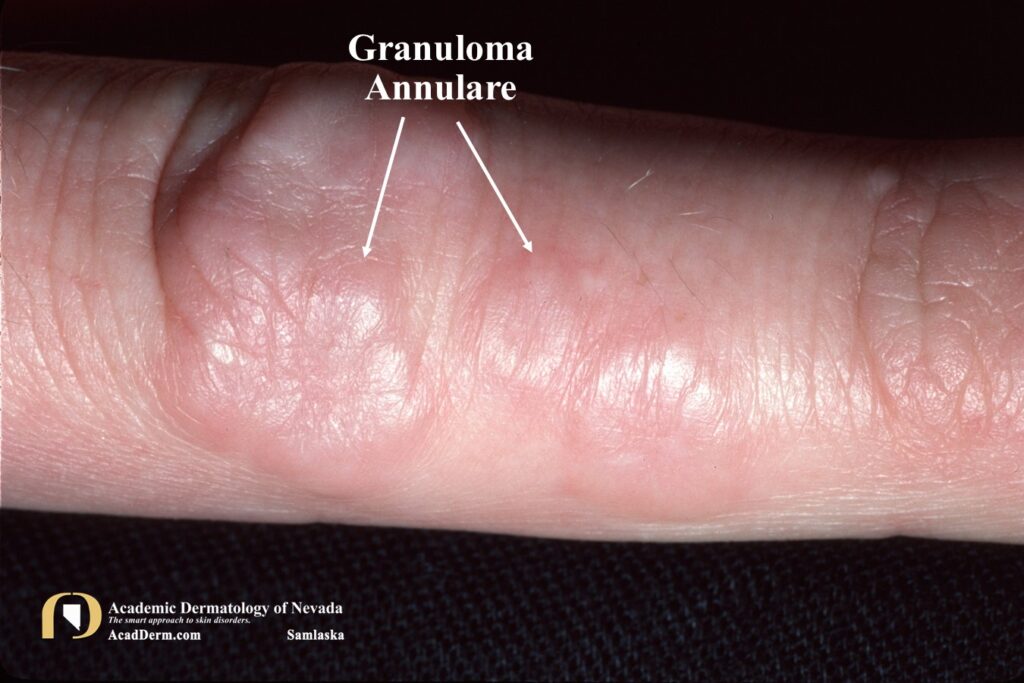
Granuloma Annulare (GA) is a common idiopathic disorder of the dermis and subcutaneous tissues. Some authors refer to it as Palisaded Granulomatous Dermatoses to encompass the many variants which include localized (most common), generalized, patch-type or macular, subcutaneous and perforating granuloma annulare. It may occur in all races and at any age but affects women twice as often as men. GA may occur at sites of trauma or inflammatory conditions, a process referred to as Koebner phenomenon. The localized form tends to afflict children and young adults and one or a few lesions are noted on presentation. The most common sites of involvement are the fingers or hands, elbows, dorsal feet and ankles. The lesions are erythematous and fawn colored or violaceous, thinly bordered plaques or papules that slowly spread peripherally while undergoing central resolution or involution, forming roughly annular lesions.
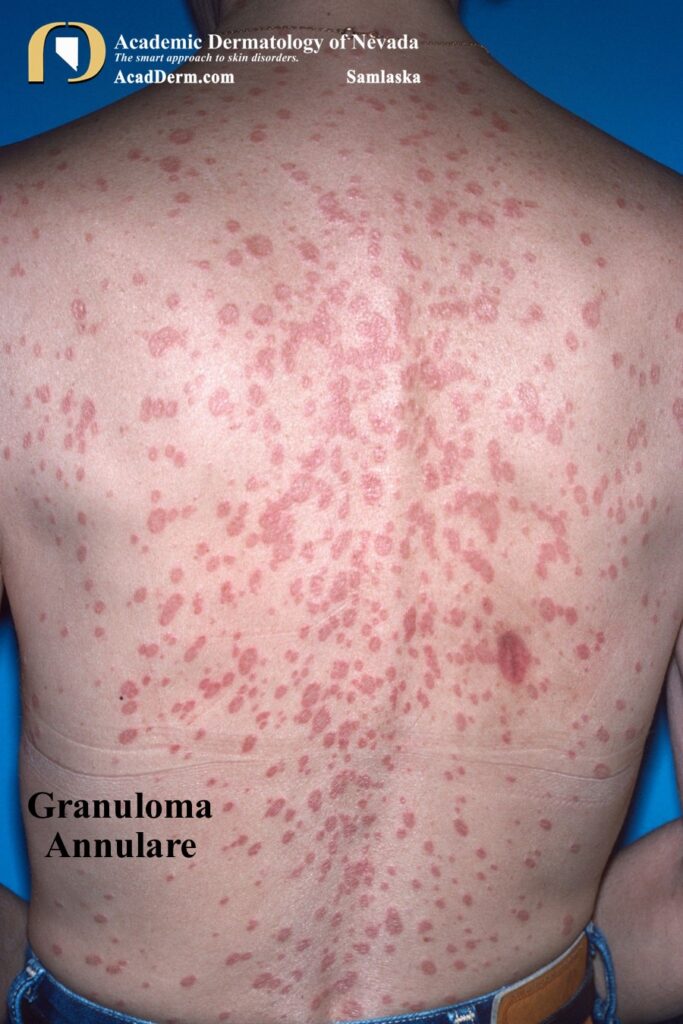
Generalized GA is defined as those patients with numerous lesions, often times involving the trunk and upper and lower extremities. Generalized GA affects mostly women in the fifth and sixth decades of life but is also a common pattern in adolescents and children. Generalized GA may be associated with diabetes mellitus, but a true association has been questioned in the literature.
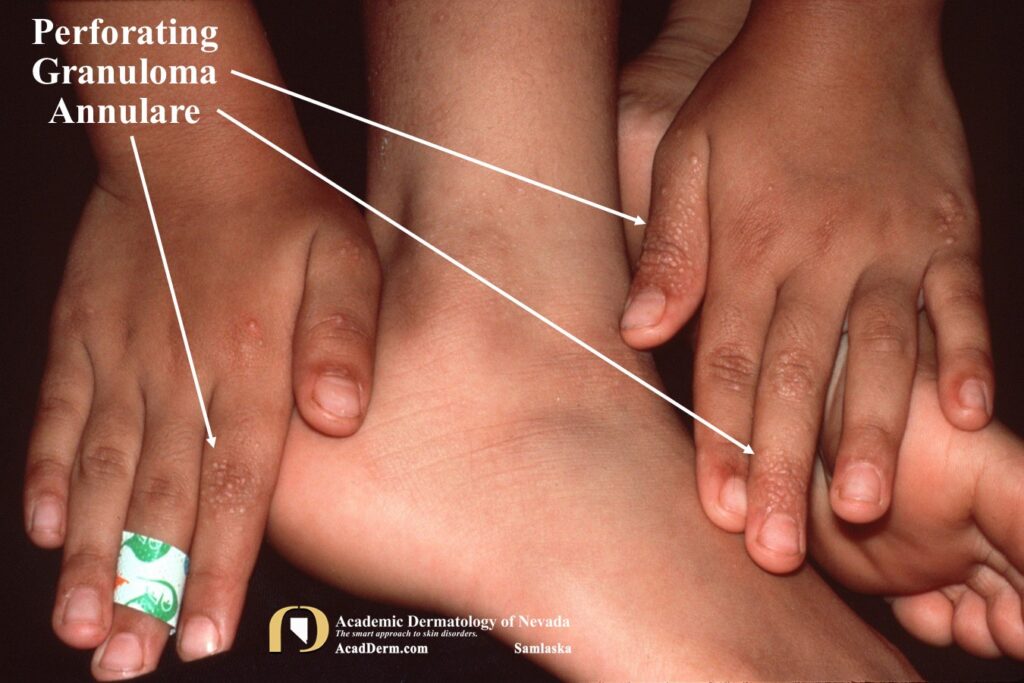
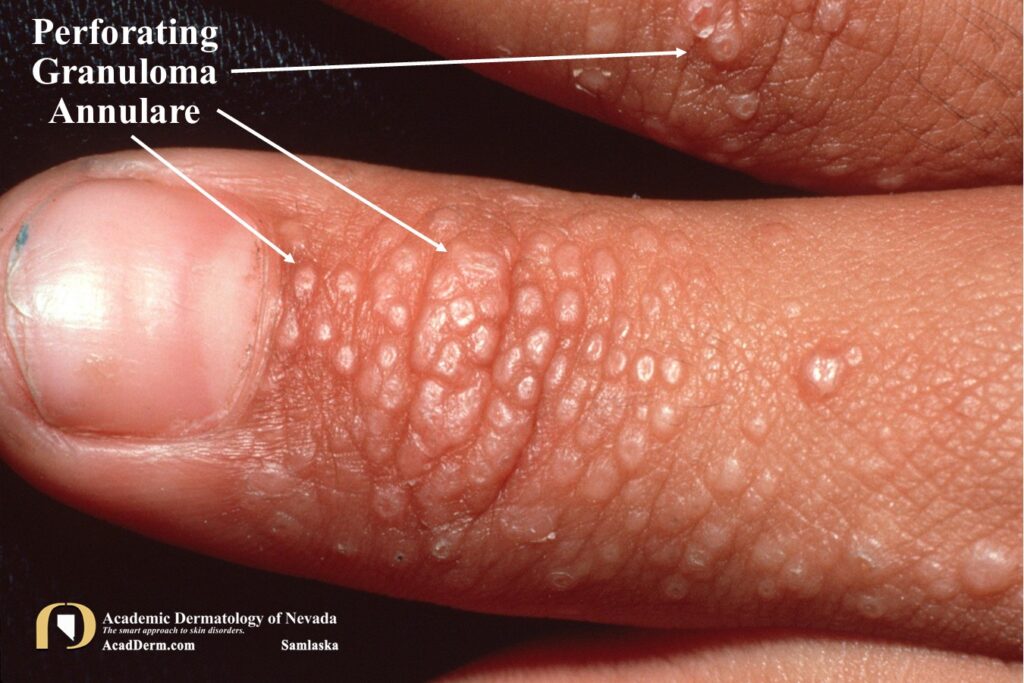

Perforating GA usually appears on the dorsal hands and presents as papules with a central keratotic core, which represents transepidermal elimination of the degenerated material in the center of the GA lesions. Clinically this can resemble a pustule.
HISTOLOGY: Classic pattern of GA is a palasading granuloma characterized by hisitiocytes and epithelioid cells surrounding a central zone of altered collagen. Mucin deposition may be present in well-developed lesions. A second pattern may be found comprised of an interstitial pattern demonstrating patchy dermal infiltrates comprised of histiocytes and other mononuclear cells with occasional neutrophils interspersed between collagen bundles.
ETIOLOGY: The cause of GA is unknown. However, the disease has been associated with diabetes mellitus, thyroid disease, mild trauma, hyperlipidemia, infections (EBV, HIV, varicella-zoster virus and tuberculosis), vaccines, malignancy and certain drugs such as TNF-alpha inhibitors. There is little evidence supporting the association with diabetes.
TREATMENT: No treatment is required, and although most lesions regress spontaneously it may take years and they tend to recur. Long-term follow-up of patients reveals that the lesions usually heal and that patients remain healthy and do not develop unusual diseases. I usually start with use of high potency topical steroids, but it should be stated that there are many treatments reported, suggesting that no one treatment is uniformly efficacious or considered the treatment of choice. Other treatment options include phototherapy, excimer or pulsed dye lasers, hydroxychloroquine, cyclosporine, methotrexate, pentoxiphylline, rifampin, ofloxacin, minocycline, dapsone, vitamin E, topical imiquimod, topical tacrolimus and oral retinoids, to name a few. To read more about GA click HERE and HERE.