In 1860 von Hebra first described Erythema Exudativum Multiforme. The original disease described is now called Erythema Multiforme Minor or Herpes Simplex Associated Erythema Multiforme and is often associated with a recurrent herpetic infections. When cutaneous lesions are accompanied with mucosal membrane involvement the cause is most often related to Mycoplasma infection (pneumonia) and is referred to as Erythema Multiforme Major. Together they are referred to as Erythema Multiforme (EM). There is a good classification scheme noted in Andrews’ Textbook of Dermatology based on treatment and prognosis:
- Herpes simplex-associated EM (HAEM)
- Erythema multiforme major (Mycoplasma)
- Chronic oral EM
- Contact dermatitis-induced EM
- Radiation-induced EM
- Idiopathic
It is more common in men with a ratio of 1:5 (M:W). The prevalence is unknown, but appears to be under 1% of the general population. The classification spectrum may include Steven’s Johnson Syndrome which appears on the most severe spectrum of EM…
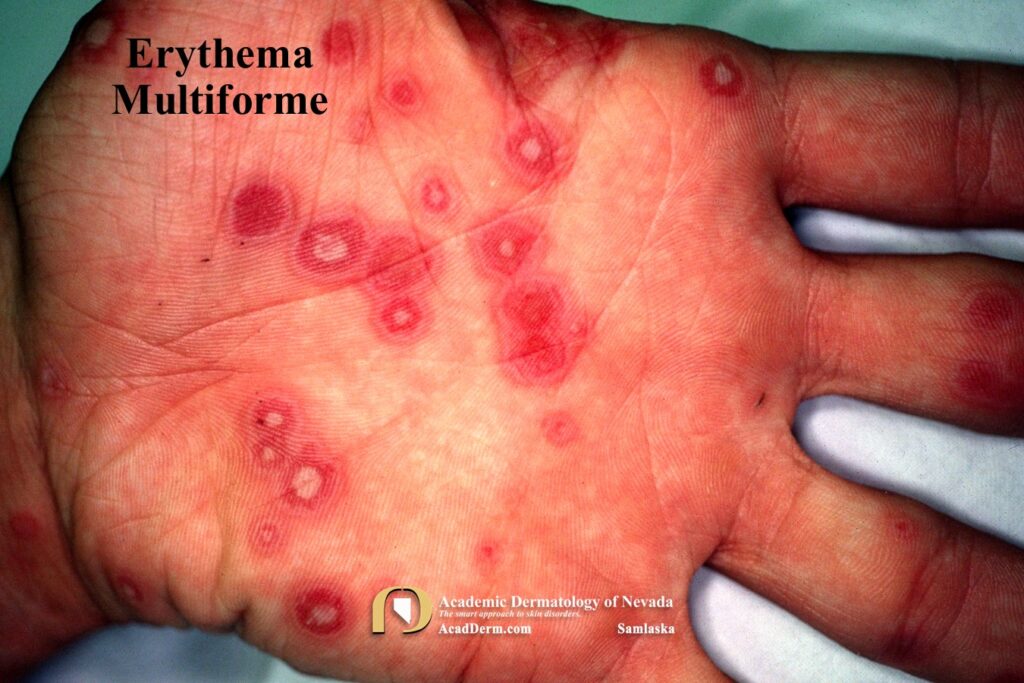

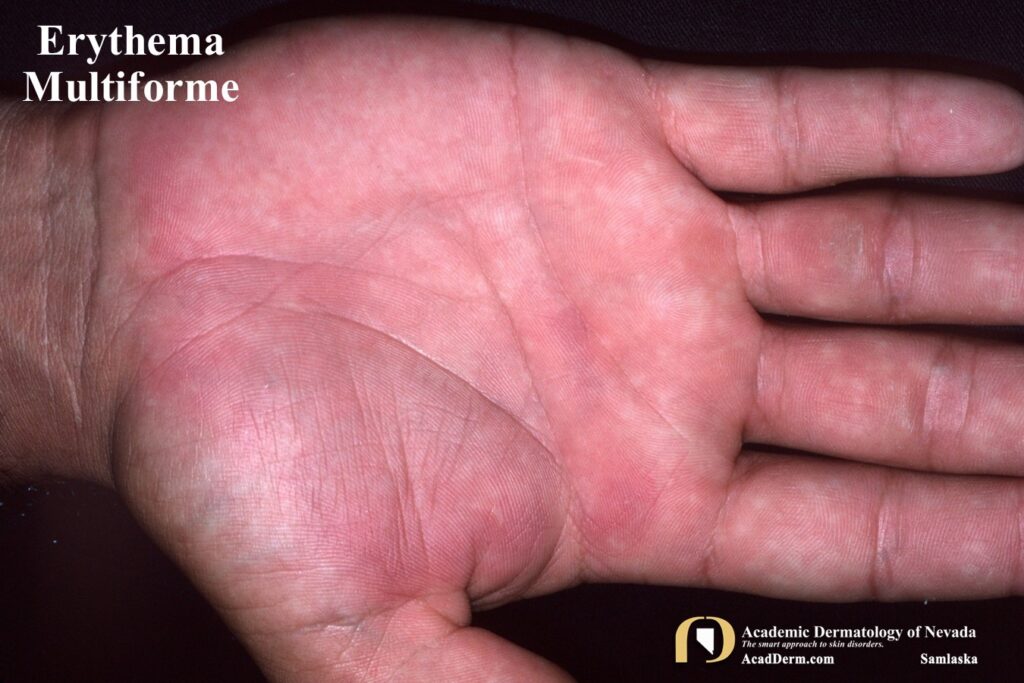

HAEM is a recurrent self-limited disease found usually in young adults, occurring seasonally in the spring and fall that often is associated with an outbreak of Herpes (cold sores; HSV-1, genital; HSV-2). The episodes often last between 1-4 weeks. The lesions are sharply marginated, erythematous macules which become palpable within 24-48 hours. The lesions are most often around 1 cm in size, but may reach several centimeters in size. Most commonly a ring of erythema forms around the periphery while the central lesion flattens and becomes purpuric or dusky–resulting in a “target” or “iris” look often referred to as “targetoid.” Targets often are found on the palms and soles but can be found more generalized.


Koebner phenomenon or photo-accentuation may occur. In children the lesions often are confused with acute urticaria as shown below. A test which may be helpful is it to draw along the margins of a few lesions. If the lesions expand beyond the ink margin in the next 30-40 minutes then the diagnosis is consistent with acute urticaria. No advancement would suggest more fixed lesions and Erythema Multiforme is the most likely diagnosis.


ETIOLOGY: As noted above, HSV-1 and HSV-2 infections are the most common cause of Erythema Multiforme Minor and Mycoplasma the most common cause of Erythema Multiforme Major. More rarely it has been reported with vaccines and medications. The most common medications associated with EM are penicillins, cephalosporins, macrolides, sulfonamides, anti-tuberculoid agents, and antipyretics. Some authors believe that it can also be associated with contact with heavy metals, herbal agents, topical therapies and poison ivy. There is also a case report of EM being induced with use of topical imiquimod 5% cream. It may occur in association with radiation therapy particularly when associated while on dilantin therapy (click HERE). EM has been reported with COVID-19 (click HERE).
TREATMENT: Medical intervention is based on severity. For most patients the disease is self-limited and requires only supportive care. For those patients with HSV triggers the treatment is designed at prevention and treatment of the HSV by use of oral agents such as valtrex. For those failing these measures dapsone, cyclosporine or thalidomide may be useful. For more information about EM click HERE, HERE and HERE. Again, as always, the information provided is for educational purposes only and is not designed to substitute for clinical evaluation by a certified dermatologist.